
Laparoscopic Mini Gastric Bypass is one of the safest and most effective surgical treatments for obesity worldwide. It helps patients achieve significant weight loss and improves many obesity related conditions such as diabetes and high blood pressure.
However, as with any surgical procedure, some potential complications may occur after Mini gastric Bypass. These complications are generally rare, especially when the procedure is performed by an experienced surgeon using modern surgical tools and techniques.
At Dr. Ahmed Shinkar Bariatric and Laparoscopic Surgery Center – Shinkar Clinic, the latest international standards in bariatric surgery are followed in order to minimize complication rates to the lowest possible levels.
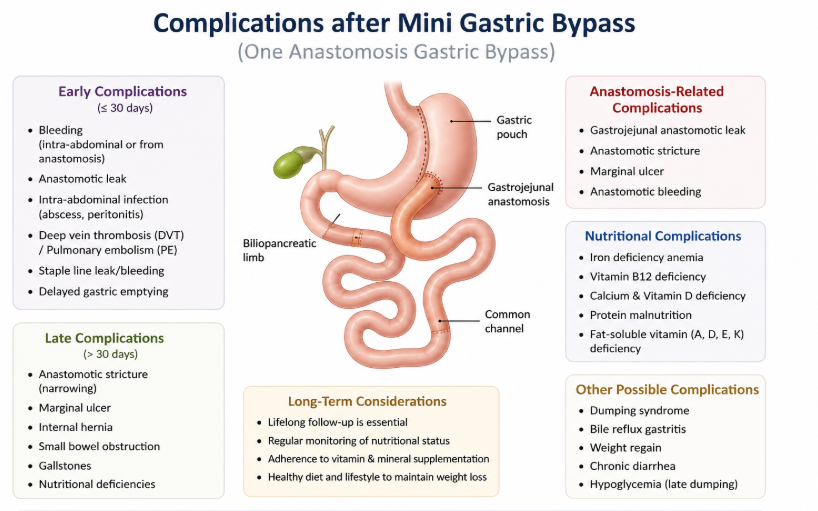
Below are the most important possible complications after Mini gastric Bypass.
Gastric Leak
A gastric leak is a rare but important complication after Mini gastric Bypass.
It occurs when part of the stomach does not heal properly after surgery, allowing gastric fluid to leak into the abdominal cavity.
A leak test is routinely performed during surgery to ensure the integrity of the stomach. However, a small international incidence remains, typically less than 0.5%.
Leaks occurring shortly after surgery are often related to failure to follow the dietary instructions during the first postoperative month.
Late leaks, which may occur months after surgery, can be associated with:
Use of painkillers (NSAIDs)
Cortisone medications
Weight-loss medications
Smoking in all forms
Excessive caffeine intake
Causes of Gastric Leak
Failure to follow the prescribed diet during the first postoperative month
Smoking (cigarettes, shisha, or electronic cigarettes)
Cannabis use or tramadol abuse, which directly affect the stomach lining
Previous abdominal operations may slightly increase the risk of leakage such as:
Gallbladder removal
Hernia repair
Abdominoplasty
Previous stomach surgery
At Shinkar Clinic, complication rates (including gastric leak) are among the lowest internationally due to adherence to international surgical standards, use of high quality stapling devices, and extensive experience with thousands of cases.
Bleeding
Bleeding may occur from the gastric staple line. The international incidence is less than 0.5%.
Bleeding is more likely in patients with:
High blood pressure
Previous abdominal surgeries
In most cases, bleeding can be treated conservatively with medication. Surgical intervention could be required only in rare cases.
Biliary Reflux
This is a rare complication of One-Anastomosis Mini Gastric Bypass (OAGB) and in most cases responds rapidly to medical treatment.
Vomiting
Vomiting may occur during the first few days after surgery, especially within the first 2-3 days, usually due to anesthesia medications or adaptation to the new stomach size.
Vomiting occurring 6-12 months after surgery may be associated with:
Smoking
Excessive use of painkillers
High caffeine intake
Sagging Skin (Loose Skin)
Loose skin may occur due to rapid weight loss.
The best way to minimize skin laxity is through regular exercise, particularly resistance and weight-training exercises.
Patients are advised to begin exercising from the third week after surgery, with workouts 3-5 times per week.
Additional recommendations include:
Consuming Whey Protein Isolate
Maintaining adequate hydration
Taking prescribed vitamin supplements
There are no creams or cosmetic treatments proven to prevent loose skin, and some patients with severe obesity may eventually require body contouring surgery.
Gallbladder and Kidney Stones
Rapid weight loss can lead to reduced gallbladder activity, increasing the risk of gallstone formation.
To prevent gallstones, patients are often prescribed Ursodeoxycholic Acid (Ursofalk) during the weight-loss phase.
Kidney stones may also develop due to:
Insufficient fluid intake
Calcium supplements that contain calcium carbonate instead of calcium citrate
Patients should drink adequate amounts of water and follow medical instructions carefully.
Blood Clots
Blood clots may occur due to:
Limited physical activity
Inadequate fluid intake
The risk is highest during the first month after bariatric surgery.
Clots may affect:
The legs (deep vein thrombosis)
The lungs (pulmonary embolism)
The intestines
Preventive medications are routinely prescribed to reduce this risk.
Splenectomy
Splenectomy (removal of the spleen) is a very rare complication of bariatric surgery.
It may occur during or after surgery due to:
Severe bleeding
Gastric leak
Abscess formation
Dense adhesions
The estimated incidence is 1–5 cases per 1000.
Anesthesia Complications
Rare anesthesia complications may include:
Allergic reactions
Pneumothorax (air leakage around the lung)
These complications are uncommon.
Mortality Risk
The international mortality rate for bariatric surgery is approximately 1 in 1000 cases.
Death (although extremely rare) may occur during or after surgery due to surgical or anesthesia related complications.
Final Advice
Possible complications should not prevent patients from seeking treatment for morbid obesity.
The complications associated with severe obesity—including:
Diabetes
Hypertension
Breathing problems
Blood clots
Stroke
Sudden cardiac death
Heart failure
Depression
Infertility
Certain cancers
are more common and often more dangerous than the complications of bariatric surgery.